Incidental CT Findings in a Patient with Influenza Type A, Admitted to the Hospital After a Syncopal Episode
Marjorie P. Zambrano, MD
Richmond University Medical Center
Case
A 58-year-old male with a past medical history of Acute Coronary Syndrome (ACS), presented to the emergency department (ED) with the chief complaint of syncope. Patient also endorsed that he was experiencing cough and fever for the past 48 hours.
On the admission day, the patient was coughing repeatedly at home. After a vigorous cough he had a syncopal episode. Right after this, the patient was brought to the emergency department (ED) and admitted for syncope workup.
Due to the patient's cough and fever, a chest x-ray was taken to rule out any infectious respiratory process, and a viral panel was performed as well. An abnormality was noted in the right bronchi (Figure 1). The shape of the right bronchi was distorted, and much more dilated in comparison with the left bronchi; which prompted us to order a computed tomography (CT) of the chest.
The computed tomography (CT) scan (Figures 2 and 3) showed suspicion for pneumomediastinum. From the right mainstem bronchus, there was a projection noted medially into the mediastinum, and there were small rounded air collections adjacent to the right main bronchi. The differential at the time was pneumomediastinum vs diverticula.
Repeated chest x-ray 5 hours after the first one was taken, it showed no active disease. It did not demonstrate progression of suspected pneumomediastinum, and bronchial diverticula was confirmed. The patient was monitored at all times with a SatO2 of 98-99% on room air and in no respiratory distress.
The patient was a non-smoker and did not take any medications or use illicit drugs. The patient was admitted for further workup for syncope, and Oseltamivir was started for Influenza type A.
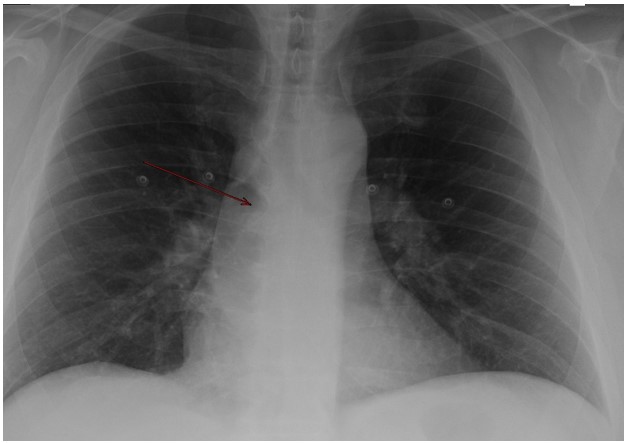
Figure 1. An abnormality in the right main bronchi on a chest x-ray (Red arrow), right main bronchi seems widened.
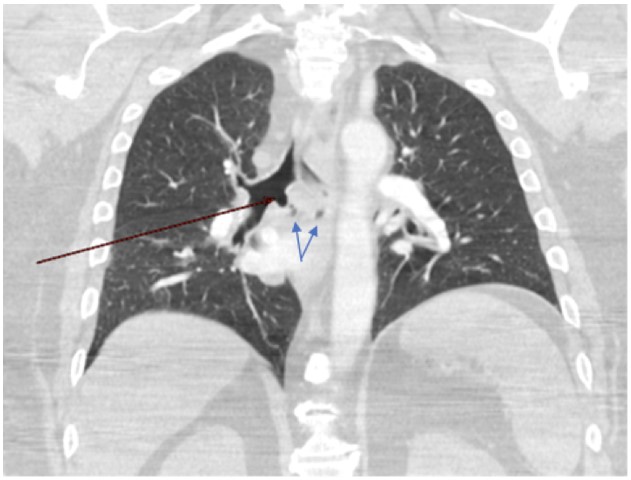
Figure 2. Computed tomography (CT) of the thorax in the coronal plane. A projection from the right mainstem bronchus medially into the mediastinum (Red arrow). Small rounded air collections adjacent to the right main bronchi (Blue arrow).
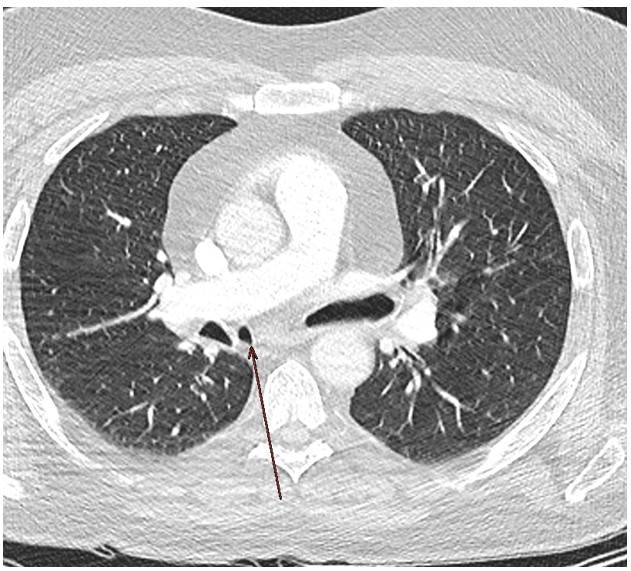
Figure 3. Computed tomography (CT) of the thorax in axial plane demonstrating the projection or outpouching from the right mainstem bronchus (red arrow)
On the physical exam, the chest wall was symmetric, without deformity. No tenderness was appreciated upon palpation of the chest wall. The patient did not exhibit signs of respiratory distress; and normal heartbeat and breath sounds were heard upon auscultation. The patient denied chest pain, and shortness of breath.
Laboratory evaluation was unremarkable, but serology revealed that the patient was positive for Influenza type A.
Question
What is a serious condition that bronchial diverticula can mimic?
- Pneumothorax
- Pulmonary edema
- Pneumomediastinum
- Cystic Fibrosis
Answer C. Pneumomediastinum
Discussion
Bronchial diverticula are projections or outpouching that are still considered as incidental and rare findings. The patients do not present with any type of symptomatology, and it has been associated with patients who have Chronic Obstructive Pulmonary Disease (COPD) (1).
Literature has described the presence of tracheal diverticula as well, and between the bronchial and tracheal, the latter has been the most common. (1,2). These outpouching have been described to be congenital or acquired. (3)
Congenital diverticula are considered a remnant of an accessory bronchus that are most likely located in the right mainstem bronchus or the lower trachea. (3) The congenital diverticula affect not only the respiratory epithelium, but also the smooth muscle and the cartilage; as seen on the congenital tracheal diverticula. (4)
The acquired diverticula are related to weakness in the wall, secondary to chronic pulmonary conditions, surgical procedures or tracheomalacia. (3,4). The outpouching of an acquired diverticula only includes the respiratory epithelium; as reported on the acquired tracheal diverticula. (4)
In 2012, a study in Italy was conducted to determine the prevalence of bronchial diverticula in non-smokers. 121 patients were enrolled, they were non-smoker participants, who had a referral to get a chest computed tomography (CT) for different reasons. (5) Most importantly, these patients did not have any respiratory symptoms when undergoing computed tomography (CT). The study reported a prevalence of 33.9%; more present in males than females, and with the right main bronchi more involved. (5)
Even though the study mentioned above showed a prevalence of 33.9%, there is no no clear prevalence of this rare disease. There have been many studies that have shown different values.
(6) These different percentages have been influenced by the type of population enrolled, for example smokers vs non-smokers. It seems that patients who have a history of smoking have a higher risk of acquiring a bronchial diverticula when compared to those who did not smoke. (7)
Regarding bronchial diverticula, the most common location as mentioned above has been the subcarinal region of the right main bronchi. (3,8) and it has been related to patients with Chronic Obstructive Pulmonary Disease (COPD), but few studies have been proven otherwise. These studies have also shown that the presence of diverticula is not a criterion for Chronic Obstructive Pulmonary Disease (COPD). (2,3,8).
In this case report, the theory was thought to be a congenital diverticula. Since the diverticula is located in the right main bronchus where most of the congenital bronchial diverticula have been reported. Also, the patient did not have a past medical history of Chronic Obstructive Pulmonary Disease (COPD) or any other type of chronic respiratory disease. This conclusion is based only on the patient's history, physical exam and early imaging, since we do not count with a bronchoscopy examination.
As seen in this case, bronchial diverticula may mimic other more serious entities such as pneumomediastinum. But not all cases of air locules outside of the trachea and bronchi are true pneumomediastinum, it will depend on the presentation of the patient. It is highly recommended to suspect other etiologies that are benign in nature, such as congenital bronchial diverticula. This is very important, to minimize unnecessary procedures and or radiation exposure, that is very well known to be related to increased morbidity and mortality.
Bronchial diverticula are mostly an incidental finding on chest computed tomography (CT), which is the best imaging modality to detect them. These diverticula are either congenital or acquired asymptomatic projections of the bronchi, and when acquired they have been highly associated with smoking.
References
-
Polverosi R, Carloni A, Poletti V. Tracheal and main bronchial diverticula: the role of CT. Radiol Med. 2008 Mar;113(2):181-9. English, Italian. doi: 10.1007/s11547-008-0249-6. Epub 2008 Apr 2. PMID: 18386120.
-
Wang NS, Ying WL. Morphogenesis of human bronchial diverticulum. A scanning electron microscopic study. Chest. 1976 Feb;69(2):201-4. doi: 10.1378/chest.69.2.201. PMID: 813965.
-
Oizumi, Satoshi M.D.; Ishida, Takashi M.D.; Kamachi, Masafumi M.D.; Takahashi, Toru M.D.; Ogura, Shigeaki M.D.; Munakata, Mitsuru M.D.; Kawakami, Yoshikazu M.D.. Congenital Bronchial Diverticulum. Journal of Bronchology: April 1999 - Volume 6 - Issue 2 - p 101-103
-
Tanrivermis Sayit A, Elmali M, Saglam D, Celenk C. The diseases of airway-tracheal diverticulum: a review of the literature. J Thorac Dis. 2016 Oct;8(10):E1163-E1167. Doi: 10.21037/jtd.2016.10.92. PMID: 27867581; PMCID: PMC5107528.
-
Ciccarese F, Garzillo G, Chiesa AM, Poerio A, Baroncini S, Bacchi Reggiano ML, Sverzellati N, Zompatori M. Incidental finding of bronchial diverticula in a non-smoker population: evaluation on thin-section CT. Monaldi Arch Chest Dis. 2016 Jun 22;81(1-2):743. doi: 10.4081/monaldi.2015.743. PMID: 27374216.
-
Miyara T, Oshiro Y, Yamashiro T, Kamiya H, Ogawa K, Murayama S. Bronchial diverticula detected by multidetector-row computed tomography: incidence and clinical features. J Thorac Imaging. 2011 Aug;26(3):204-8. Doi: 10.1097/RTI.0b013e3181ebedc4. PMID: 20818276.
-
Johaness Gossner. Prevalence of main bronchial diverticula in a general European population. European Journal of anatomy. ISSN 2340-311X (Online)
-
Higuchi T, Takahashi N, Shiotani M, Sato S, Ohta A, Maeda H, Nakajima H, Itoh K, Tsukada H. Main bronchial diverticula in the subcarinal region: their relation to airflow limitations. Acta Radiol. 2012 Feb 1;53(1):44-8. doi: 10.1258/ar.2011.110222. Epub 2011 Nov 8. PMID: 22067207.


