A Deadly Load
Arnav Gupta, MD; Pulmonary/Critical Care Fellow, University of Colorado School of Medicine Division of Pulmonary Sciences and Critical Care Medicine
Anna Neumeier, MD; Assistant Professor, University of Colorado School of Medicine Division of Pulmonary Sciences and Critical Care Medicine
Case
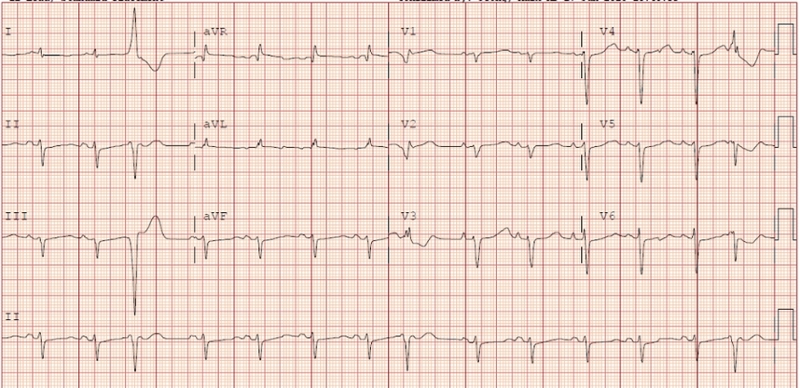
A 68-year-old man with atrial fibrillation who was admitted after elective cardioversion for dofetilide loading collapsed while ambulating. Initially he had no pulse so CPR was initiated immediately. With defibrillation, he had return of spontaneous circulation. An EKG was obtained:
Question
What does this EKG demonstrate?
- Acute anterior wall myocardial infarction
- Second-degree AV block
- QT prolongation
- Low voltage suggestive of cardiac tamponade
Answer: C. QT Prolongation
Discussion
This patient developed cardiac arrest secondary to Torsades de Pointes (TdP), a polymorphic ventricular tachycardia associated with QT interval prolongation that resulted from dofetilide. TdP is a polymorphic ventricular tachycardia described and named for its characteristic twisting of the QRS complex around a single isoelectric point on electrocardiography. TdP is pathophysiologically dependent on three conditions: prolongation of the QT interval (due to medications or congenital abnormalities); development of an early after-depolarization (a depolarization in the cell membrane that occurs prior to repolarization of the membrane and prior to the refractory period); and tissue heterogeneity that allows this early after-depolarization to propagate as an action potential in a re-entrant pathway.
Prolongation of the QT interval most commonly occurs in the acquired form due to medications that block the delayed potassium rectifier channels that are responsible for ventricular repolarization. Dofetilide is a class III anti-arrhythmic that functions by blocking potassium rectifier channels. Dofetilide can induce Tdp via prolongation of the repolarization interval as well as by slowing the heart rate. Additionally, in patients with atrial fibrillation, after restoration of sinus rhythm, there is increased risk for Tdp due to bradycardia and heightened sensitivity to QT prolonging effects of dofetilide.
Treatment of drug-induced Tdp centers on shortening the QT interval and preventing early after-depolarizations by removing any reversible causes. The precipitating drug should be stopped and electrolyte abnormalities corrected including hypokalemia (to replete intracellular potassium) and magnesium (to block calcium influx which prolongs phase II of the action potential). As QT duration is inversely correlated with heart rate, increasing the heart rate with beta-adrenergic infusions or overdrive pacing can be therapeutic when bradycardia is present.
References:
-
Yap, Y. G. Drug induced QT prolongation and torsades de pointes. Heart 2003; 89(11): 1363-1372.
-
Brumberg et al. Frequency of toxicity with chemical cardioversion of atrial fibrillation with dofetilide. Am J Cardiol 2013; 112(4): 505-8.


